
When CSCR becomes something more: a multimodal imaging case
A 57-year-old man was reviewed having received 18 intravitreal bevacizumab (Avastin) injections to the left eye over a period of approximately two years. He had a longstanding history of central serous chorioretinopathy (CSCR), and the original working diagnosis was CSCR with secondary choroidal neovascularisation. Despite treatment he had maintained partial but incomplete response, with visual acuity of 6/6 right and 6/15 left, improving to 6/9.5 with pinhole. Multimodal imaging including fluorescein angiography, indocyanine green angiography, OCT angiography, and structural OCT was performed to characterise the membrane and exclude polypoidal features.
Macular OCT - right eye. No significant pathology, but the choroid is visibly thickened with dilated outer choroidal vessels in Haller’s layer - the pachychoroid substrate present bilaterally.
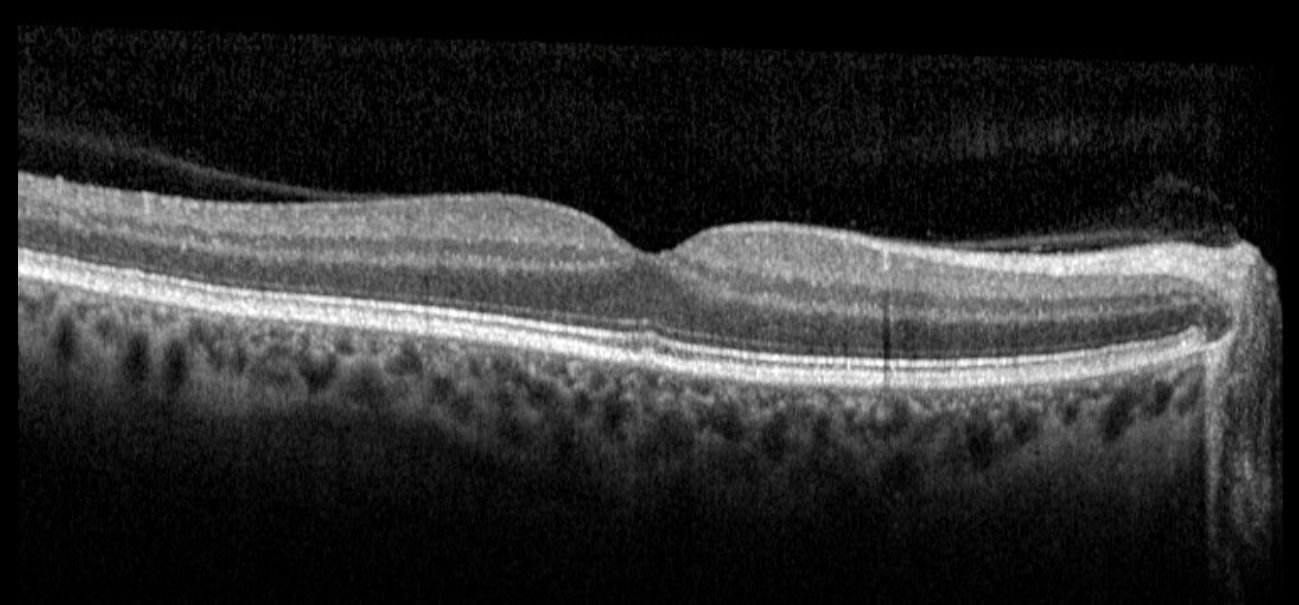
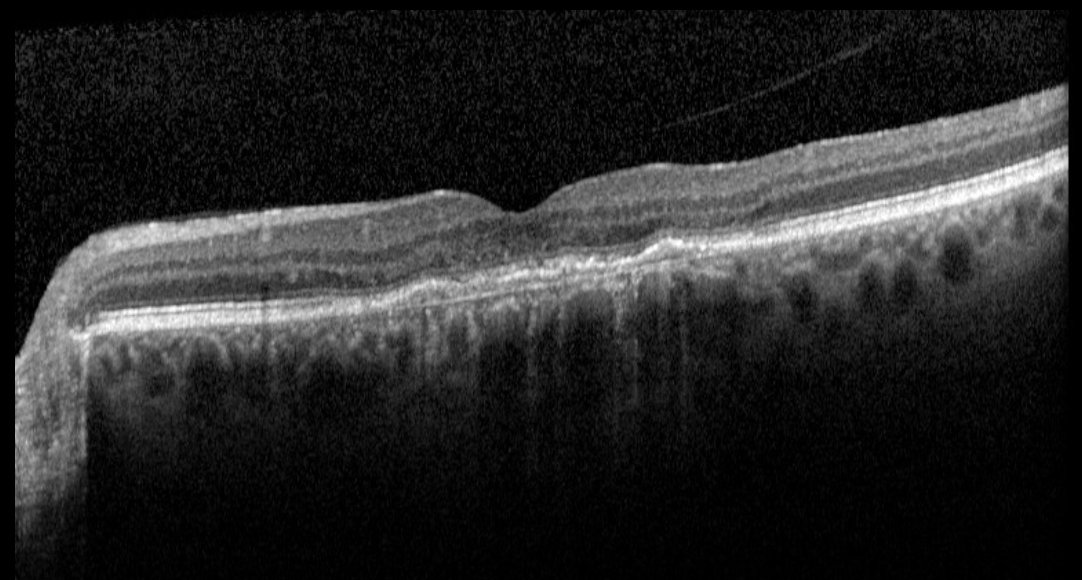
Macular OCT - left eye, prior to Eylea loading. An irregular, shallow pigment epithelial detachment with subretinal hyperreflective material overlying a markedly thickened choroid with prominent dilated Haller’s layer vessels. The double layer sign is visible - two hyperreflective bands representing the RPE above and Bruch’s membrane below, with hyperreflective CNV tissue occupying the intervening space - a useful OCT pointer to sub-RPE neovascularisation.
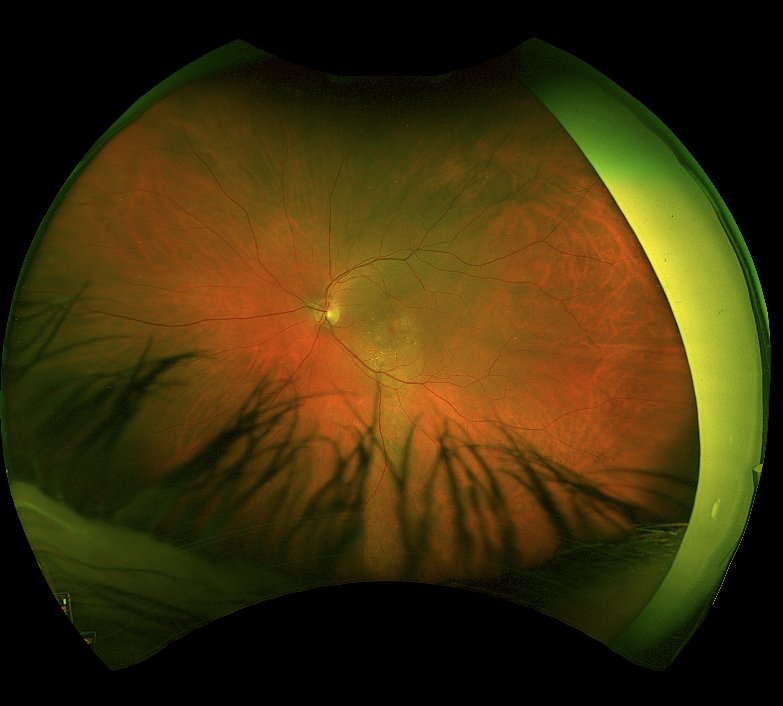
Widefield colour fundus photograph - left eye. A gravitational tract of RPE pigment change tracking inferiorly from the fovea - the hallmark of longstanding chronic CSCR with recurrent subretinal fluid tracking under gravity over years.
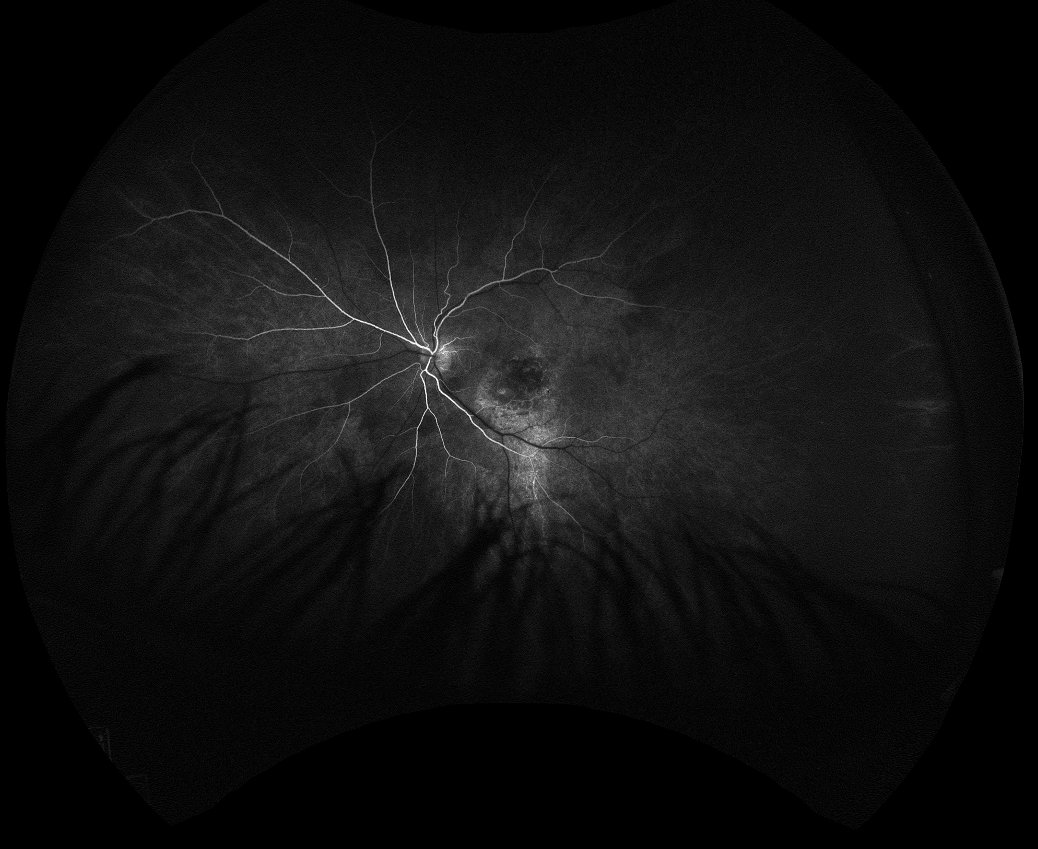
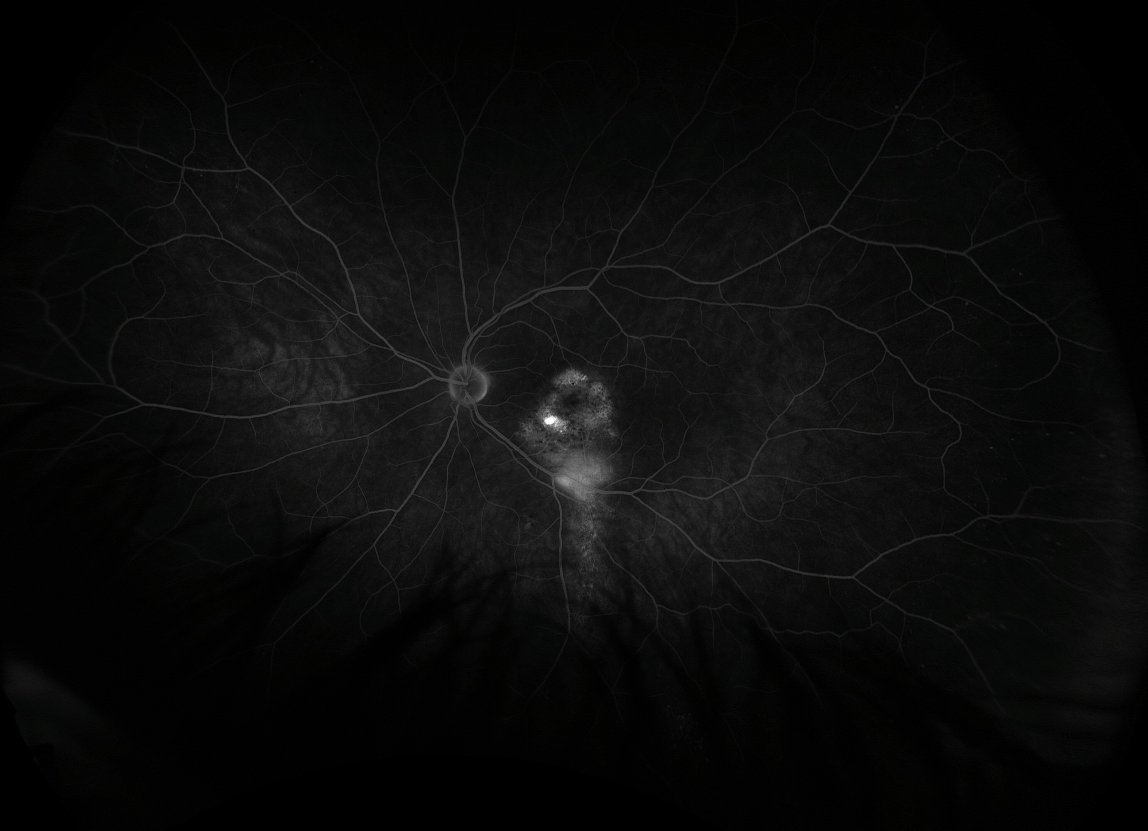
Fluorescein angiography - left eye, early phase (17 seconds). No well-defined early hyperfluorescence at the fovea, consistent with a sub-RPE type 1 neovascular membrane that does not fill early on FFA.
Fluorescein angiography - left eye, late phase (9 minutes). Ill-defined late staining at the fovea - the characteristic FFA appearance of type 1 (occult) choroidal neovascularisation, without the well-defined early leakage of a type 2 (classic) membrane.

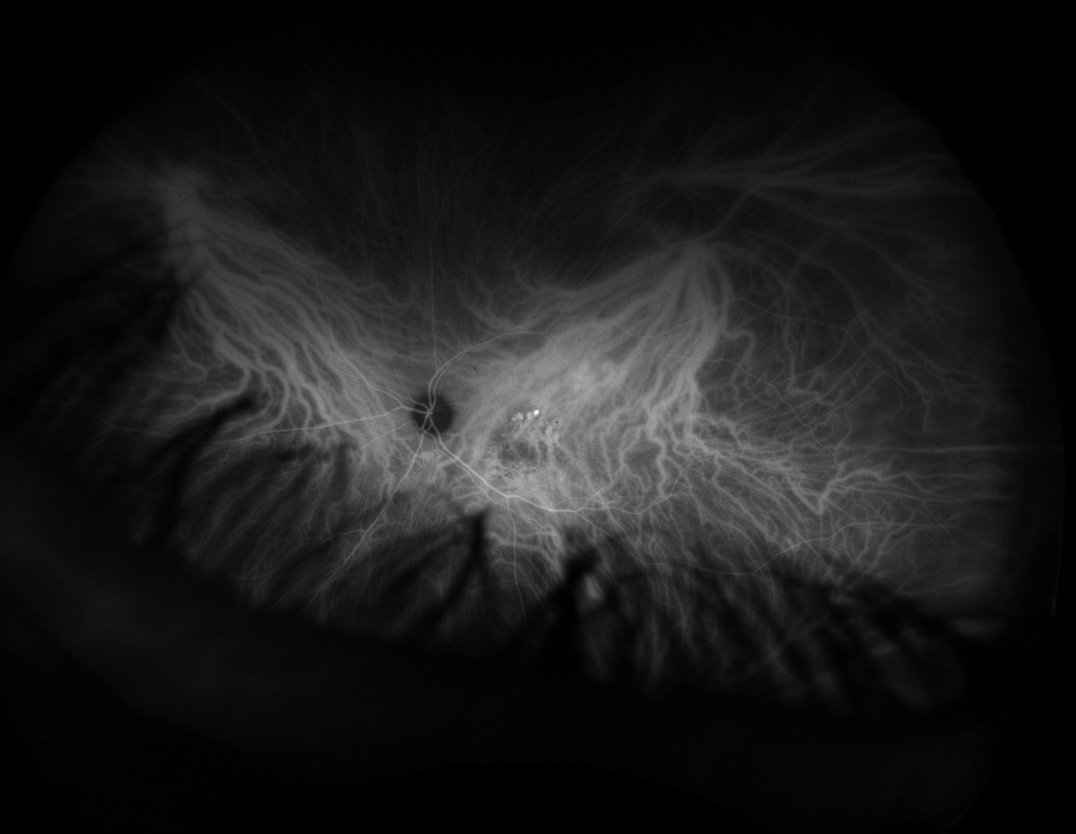
ICG angiography - left eye, early phase (20 seconds). Prominent early filling of dilated choroidal pachyvessels - the hallmark of choroidal vascular congestion in the pachychoroid spectrum.
ICG angiography - left eye, mid phase (4 minutes). The type 1 CNV network becoming visible as a lacy plaque beneath the RPE, distinct from the underlying pachyvessels.
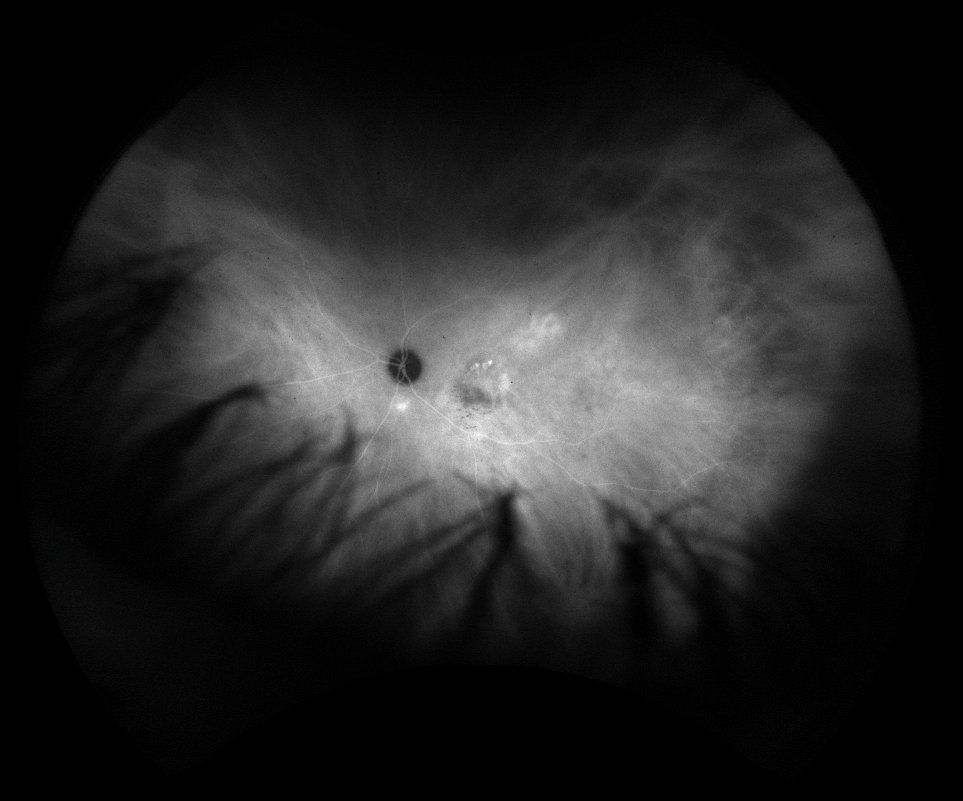
ICG angiography - left eye, late phase (10 minutes). Persistent staining of the CNV network with no focal polypoidal hot spots - polypoidal choroidal vasculopathy excluded.
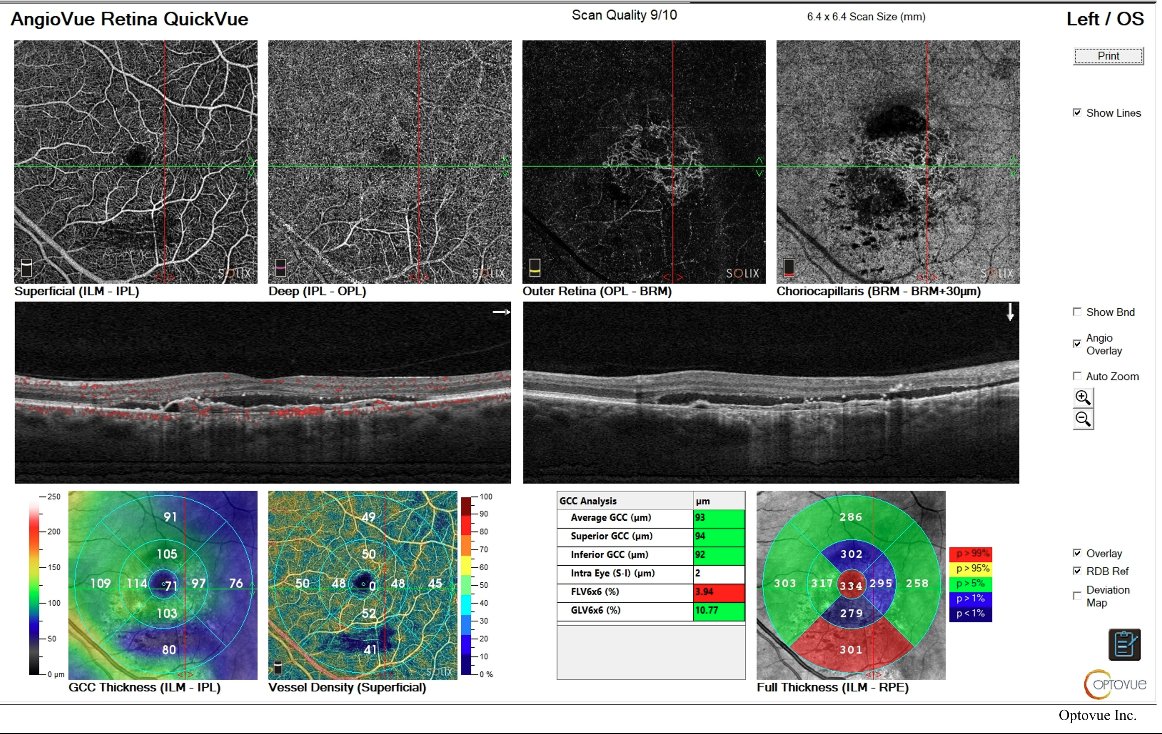
OCT angiography - left eye. The outer retinal slab demonstrates a lacy neovascular network confined to the sub-RPE space, consistent with type 1 CNV. Dilated choroidal pachyvessels visible at the choriocapillaris level.
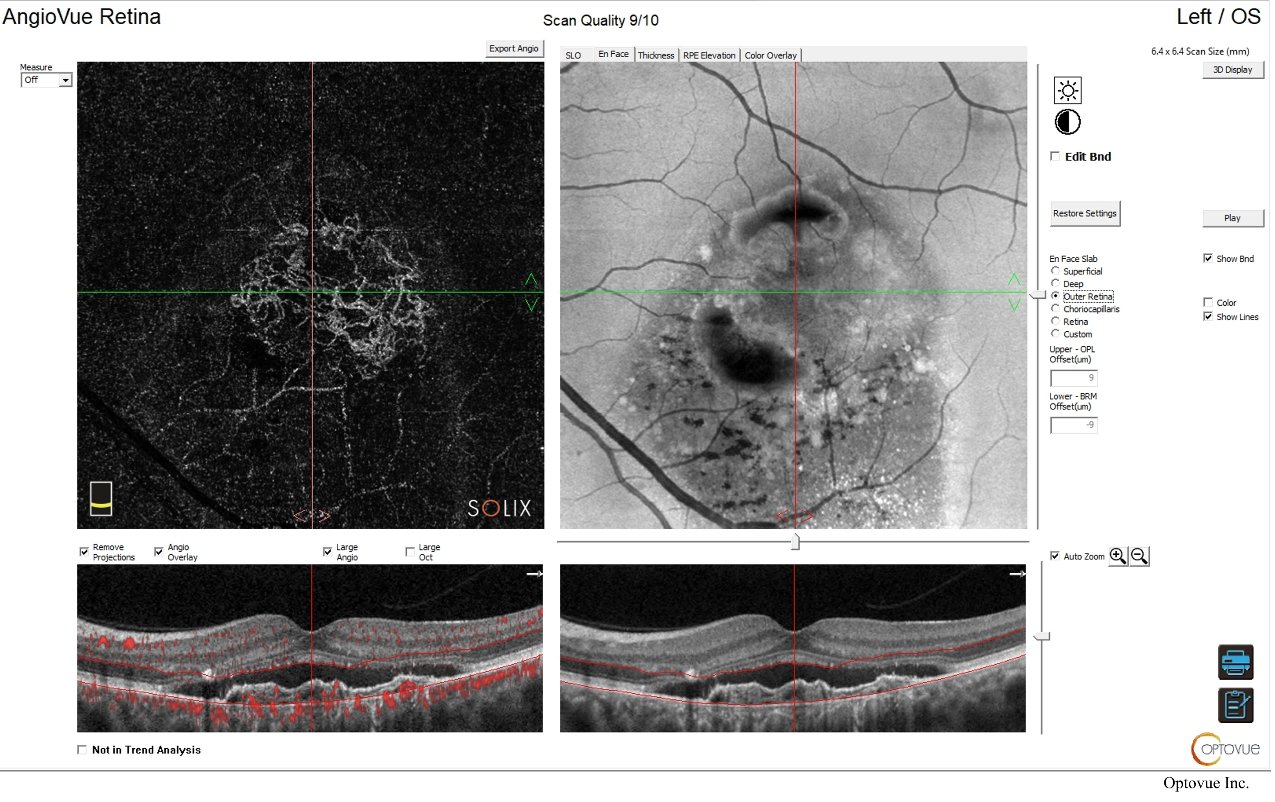
OCT angiography - outer retinal slab, left eye. The type 1 CNV network shown in detail - a characteristic frond-like configuration with no flow signal above the RPE, confirming sub-RPE location.
The multimodal imaging confirmed a type 1 choroidal neovascular membrane with no polypoidal features and a markedly thickened choroid with dilated choroidal pachyvessels - the characteristic substrate of pachychoroid neovasculopathy (PNV) , first described by Pang and Freund in 2015. PNV sits at the intersection of chronic CSCR and neovascular disease within the pachychoroid spectrum - a recognised progression pathway in which longstanding choroidal congestion and RPE stress drive the development of type 1 neovascularisation beneath the RPE, as reviewed by Kaye, Boon et al. (Prog Retin Eye Res 2020) . The gravitational RPE pigment track visible on the colour fundus photograph documents the years of recurrent CSCR activity that preceded the neovascular complication. The double layer sign on structural OCT - two hyperreflective bands with CNV tissue between the RPE and Bruch’s membrane - is a useful pointer to sub-RPE neovascularisation, though it is not specific to PNV and occurs equally in AMD with occult type 1 CNV; the key distinguishing features here are the thick choroid, dilated choroidal pachyvessels, absence of drusen, and the CSCR history. The FFA demonstrates the characteristic late staining of a type 1 occult membrane; the ICG beautifully shows both the dilated choroidal pachyvessels and the sub-RPE CNV network and confirms the absence of polypoidal hot spots; and the OCT angiography demonstrates the frond-like CNV network confined to the sub-RPE space. The absence of drusen or AMD-related degenerative change, combined with the pachychoroid substrate and the CSCR history, points firmly away from neovascular AMD. It is worth noting that the original working diagnosis - CSCR with secondary CNV - and the refined diagnosis of PNV are, in this context, essentially two descriptions of the same entity: the former describing the clinical sequence, the latter the underlying morphological substrate. PNV is now the preferred label for this presentation within the pachychoroid framework.
After 18 bevacizumab injections the membrane remained active, and the decision was taken to switch to intravitreal aflibercept (Eylea). The rationale for switching anti-VEGF agents in cases of suboptimal response is well established: aflibercept has a higher binding affinity for VEGF-A and additionally binds placental growth factor (PlGF), which may be relevant in pachychoroid-driven neovascularisation. A loading course of three monthly Eylea injections was given, followed by a treat-and-extend regimen.
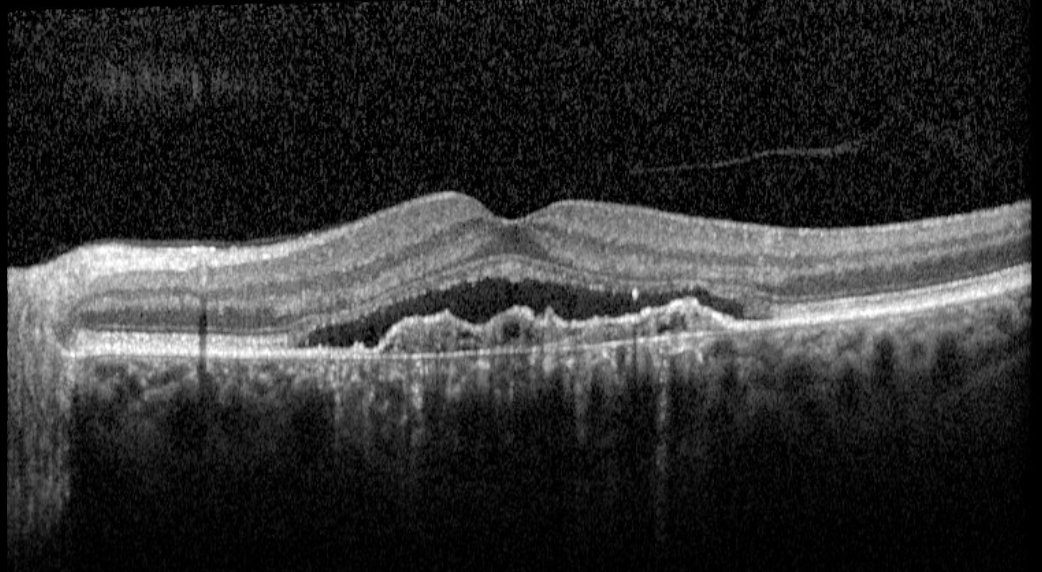
Macular OCT - left eye, four weeks after completion of three monthly Eylea injections. Significant flattening of the pigment epithelial detachment with resolution of the subretinal hyperreflective material. Visual acuity improved to 6/7.5.
The post-loading OCT demonstrates a satisfying response - the PED has flattened significantly and the SRHM has resolved. Visual acuity improved to 6/7.5 and the patient has subsequently maintained good disease control on a treat-and-extend schedule. This case illustrates how PNV can be misclassified as neovascular AMD, and how recognition of the pachychoroid substrate - thickened choroid, dilated choroidal pachyvessels, type 1 CNV without drusen, and a history of CSCR - can refine both the diagnosis and the treatment strategy.