
Loss of vision after an elective procedure
A 40-year-old woman was referred for urgent ophthalmology review following elective endovascular retreatment of a known left paraophthalmic internal carotid artery aneurysm. The aneurysm had originally been discovered and coiled without complication at the same centre in 2018, when she was 33. Neck recurrence was identified on surveillance imaging, and after discussion in a joint neurovascular clinic she elected retreatment. The coiling procedure was performed on 12 February 2026; she woke from the procedure with complete loss of vision in the left eye. On ophthalmological review the following morning, visual acuity was 6/6 right and no perception of light left, with a left relative afferent pupillary defect (RAPD). Anterior segment examination was normal.

Widefield colour fundus photograph - left eye, February 2026. Extensive retinal whitening across the posterior pole with a cherry red spot at the fovea and early disc pallor. A zone of relative preservation temporal to the disc is consistent with a patent cilioretinal artery.
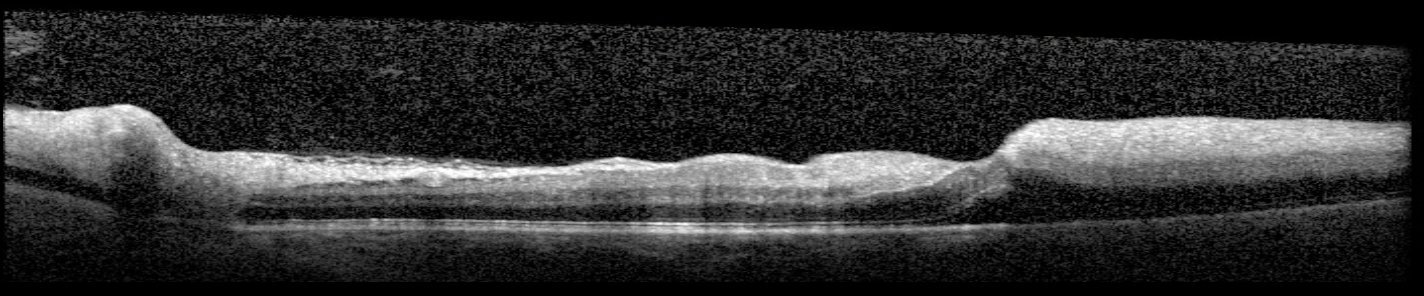
Macular OCT - left eye, February 2026. Marked hyperreflectivity and thickening of the inner retinal layers consistent with acute ischaemia, with a zone of relative preservation in the cilioretinal artery territory (corresponding with the fundus image above). The outer retinal layers are relatively preserved at this early stage.

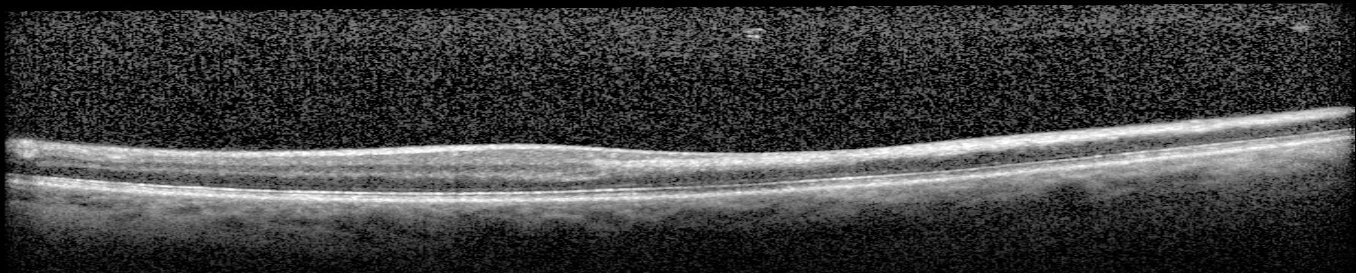
Macular OCT - right eye, February 2026. Normal retinal architecture shown for comparison.
Macular OCT - left eye, May 2026. Severe atrophy of the inner retinal layers replacing the acute oedema seen three months earlier, with marked thinning of the ganglion cell and inner plexiform layers. The characteristic appearance of chronic central retinal artery occlusion.
The left fundus showed extensive retinal whitening with a cherry red spot at the fovea and early disc pallor. A zone of relative preservation temporal to the disc is consistent with a patent cilioretinal artery - a branch of the posterior ciliary circulation rather than the central retinal artery, present in approximately a quarter of eyes, which can be spared in CRAO . The multimodal imaging features of cilioretinal artery sparing in CRAO are well illustrated in a case report by Ribeiro et al. (Ophthalmology Retina 2022) , showing the corresponding zone of inner retinal preservation on OCT and the preserved capillary plexus on OCT angiography. However, despite apparent cilioretinal sparing, the patient had no perception of light - a finding more severe than might be expected with a patent cilioretinal artery, and raising the possibility of concurrent ischaemic optic neuropathy from posterior ciliary artery microembolism during the same procedural event. The early disc pallor visible on fundoscopy within 24 hours is consistent with optic nerve ischaemia contributing to the visual loss.
MRA head performed on the evening of the procedure showed no large vessel occlusion, no carotid or vertebral dissection, and no diffusion restriction to suggest cerebral infarction - consistent with microembolism to the ophthalmic arterial circulation rather than a proximal vascular event. The paraophthalmic segment of the internal carotid artery is the site of origin of the ophthalmic artery, making aneurysms in this location and interventions here particularly vulnerable to causing embolic occlusion of the ophthalmic or central retinal artery. By the time of ophthalmological review the following morning, the window for any acute intervention had passed and nothing could be done to restore vision. The patient was counselled and discharged home pending neurovascular MDT discussion.
The serial OCT images illustrate the two phases of CRAO with particular clarity. In the acute phase, inner retinal ischaemia produces oedema and hyperreflectivity of the nerve fibre, ganglion cell, and inner plexiform layers - the retina appears thick and bright on OCT. By three months, the oedema has resolved but is replaced by severe inner retinal atrophy: the same layers are now markedly thin, representing irreversible loss of the ganglion cells and their axons. The outer retina and RPE, supplied by the choroidal circulation rather than the central retinal artery, are relatively preserved throughout. Comparison with the normal right eye OCT makes the extent of the left inner retinal loss immediately apparent.
This case is a reminder that CRAO is the ocular equivalent of a cerebral stroke - sudden, devastating, and largely irreversible once established. In a procedural context such as this, it serves as a sobering illustration of the proximity of the ophthalmic arterial supply to common neurovascular intervention sites, and the permanence of retinal ischaemia when the window for treatment has passed.