
Full-thickness macular hole with reassuring fellow eye OCT
A 64-year-old woman was referred following a routine sight test at which her right best corrected visual acuity had dropped to 6/30. She had no symptoms of floaters or flashes. The optometrist identified a full-thickness macular hole on right fundus examination and performed bilateral macular OCT. Left visual acuity was 6/6. Intraocular pressures were normal bilaterally.
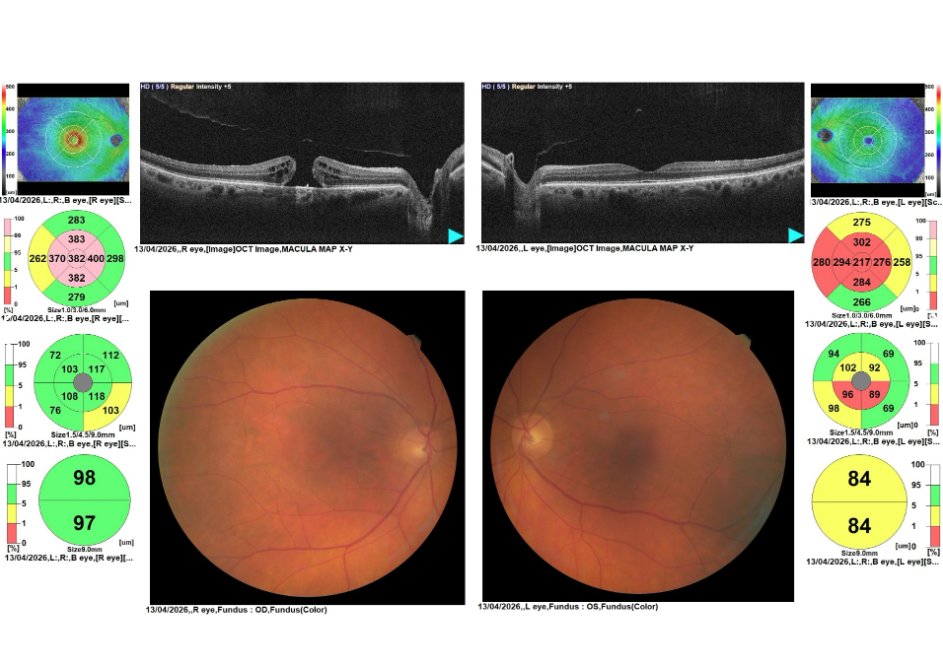
Bilateral macular OCT with thickness maps and colour fundus photographs. Right eye: full-thickness macular hole with cystic change at the hole margins and a cuff of subretinal fluid. Left eye: flat foveal contour with no hole or traction; the OCT appearance is consistent with a complete posterior vitreous detachment.
The right OCT confirms a full-thickness macular hole with cystic intraretinal changes at the hole margins and a surrounding cuff of subretinal fluid - appearances consistent with an idiopathic macular hole, most likely formed following vitreomacular traction during posterior vitreous detachment (PVD). The left OCT is reassuring: the flat foveal contour and absence of vitreomacular adhesion are consistent with a PVD already having occurred in that eye, which significantly reduces the risk of the left eye developing a hole.
The diagnosis is an idiopathic right full-thickness macular hole. The absence of floaters or flashes is a reminder that macular hole formation is not always symptomatic in the way that a peripheral retinal tear might be - central visual loss may develop gradually and go unreported until picked up at a routine test.
This patient will be seen in a surgical retina clinic within eight weeks to discuss pars plana vitrectomy . Surgical success rates for idiopathic macular hole closure are high, and earlier intervention generally carries a better visual prognosis. This case illustrates two benefits of performing OCT at the point of referral - it allowed direct routing to the vitreoretinal team rather than a general macular clinic, and it provided immediate reassurance about the fellow eye by confirming an already complete left PVD.