
A vitelliform lesion with a vascular clue
An 87-year-old woman was referred urgently by her optometrist with a working diagnosis of right vitelliform macular dystrophy and dot and blot haemorrhages on the superior and inferior arcades, with a query of underlying systemic vascular disease. Visual acuity measured 6/18 right and 6/6 left, with significantly reduced right near vision (N14 vs N5 left). Intraocular pressures were normal bilaterally.
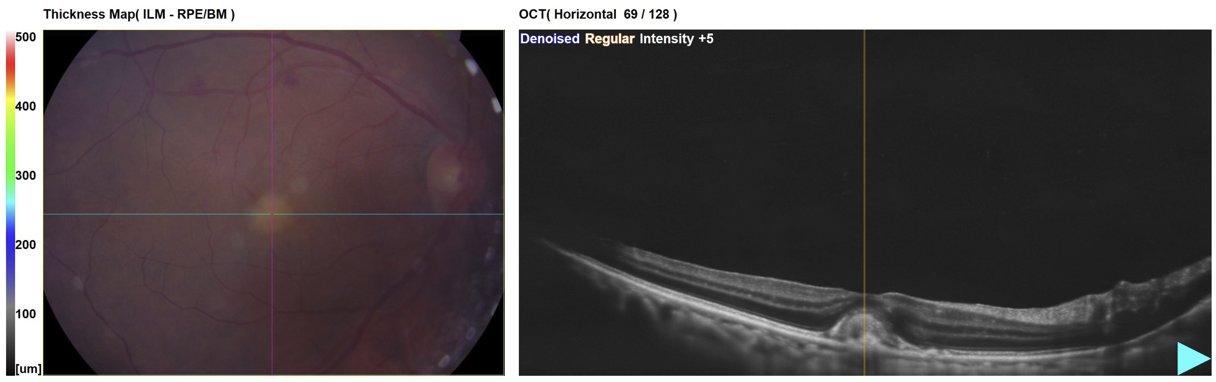
Macular OCT with thickness map - right eye. The fundus image shows scattered intraretinal haemorrhages in a sectoral distribution consistent with a superotemporal branch retinal vein occlusion. The OCT demonstrates a dome-shaped hyperreflective vitelliform lesion at the fovea with a subtle epiretinal membrane on the inner retinal surface. No subretinal or intraretinal fluid.
The right fundus photograph shows a sectoral distribution of intraretinal haemorrhages consistent with an old superotemporal branch retinal vein occlusion (BRVO) . The OCT reveals an acquired vitelliform lesion at the fovea with a subtle overlying epiretinal membrane (ERM). A plausible unifying sequence is BRVO leading to secondary ERM formation, with the ERM then causing mechanical separation of the photoreceptors from the RPE, impairing RPE phagocytosis of shed outer segments and resulting in their accumulation as a vitelliform-type deposit - a mechanism described by Govetto et al. (Am J Ophthalmol 2017) in the context of tractional abnormalities of the central foveal bouquet. This case therefore has a single plausible unifying explanation rather than three separate pathologies, though the sequence remains partly speculative.
The optometrist’s differential of inherited vitelliform macular dystrophy deserves consideration. Vitelliform maculopathy encompasses a wide range of aetiologies - as reviewed in Survey of Ophthalmology (2023) - including Best disease, adult-onset foveomacular vitelliform dystrophy, AMD-associated vitelliform change, and secondary acquired lesions as in this case. Left macular imaging was not provided with this referral. Imaging the fellow eye is always informative - the presence or absence of drusen, choroidal thickness, and any contralateral vitelliform change all contribute meaningfully to the differential, and symmetric bilateral lesions would shift the balance towards an inherited dystrophy.
The optometrist also correctly flagged the need for vascular risk factor screening - a positive step, as this is recommended for all patients with RVO in line with RCOphth guidelines . Standard initial investigations include blood pressure measurement, serum glucose or HbA1c, full blood count, and ESR. This patient will be seen in a medical retina clinic within 12 weeks, with periodic OCT review planned to monitor ERM progression, conversion of the vitelliform lesion to atrophy, or development of secondary choroidal neovascularisation.