
Focal choroidal excavation: an incidental OCT finding in a young patient
A 27-year-old man was seen for his first routine sight test. He had no visual symptoms. Visual acuity was 6/6 bilaterally with no refractive error. Intraocular pressures were 18 mmHg right and 17 mmHg left. The optometrist performed an OCT and noted an area of apparent RPE absence inferonasal to the right optic disc, querying whether the patient needed to be seen or could be monitored in the community.
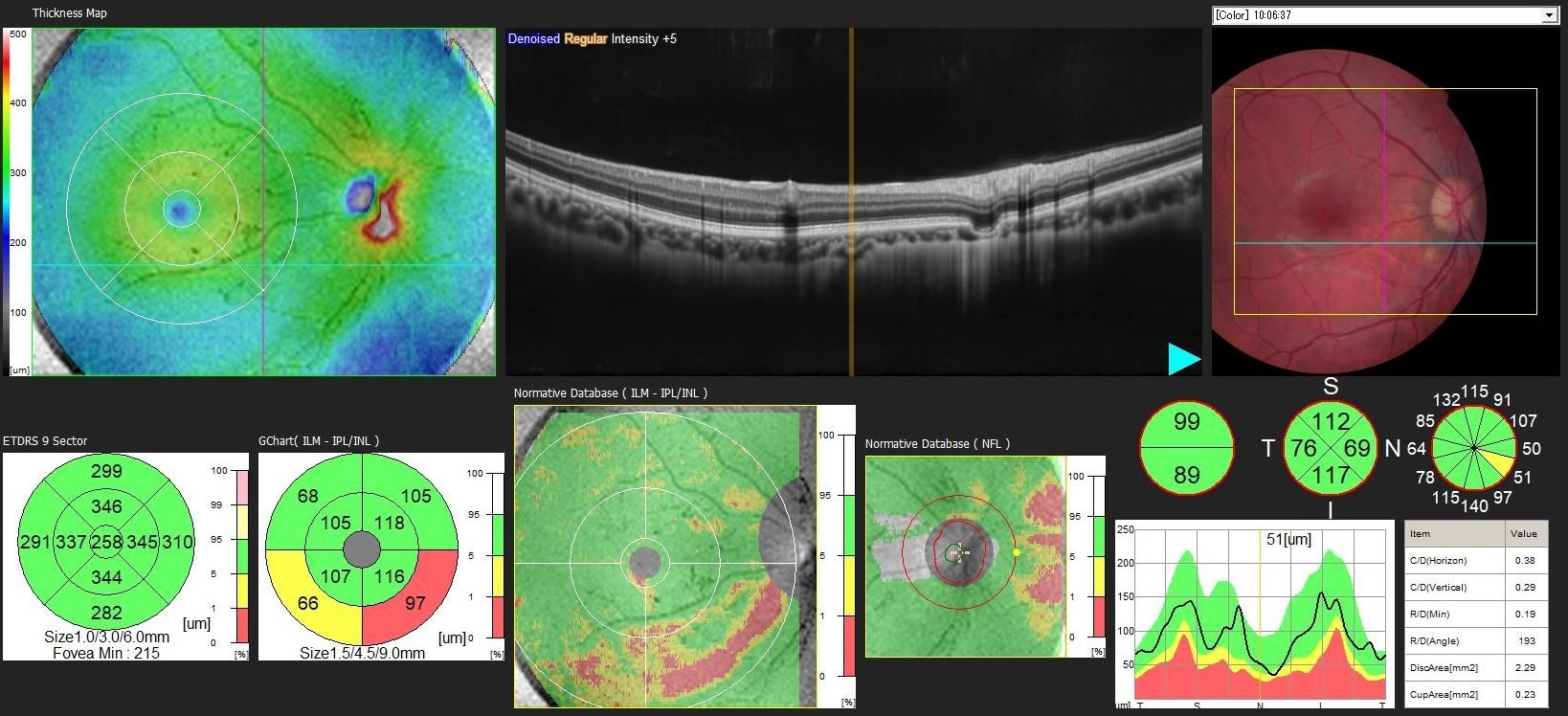
Macular OCT with thickness map and colour fundus photograph - right eye. A focal excavation of the choroid is visible inferonasal to the fovea, with the overlying RPE and outer retinal layers conforming to the contour of the depression. No subretinal fluid. The thickness map confirms focal thinning at the corresponding location.
The OCT appearance is typical of a focal choroidal excavation (FCE) - a rare, idiopathic, localised pit or depression within the choroid, first described by Jampol et al. in 2006 and later characterised in detail by Margolis et al. (Arch Ophthalmol 2011) . The excavation in this case is conforming - the photoreceptors follow the RPE contour without a subretinal gap, distinguishing it from the non-conforming subtype in which a space exists between the RPE and the photoreceptor tips. The optometrist’s description of apparent RPE absence is an understandable interpretation of this appearance on OCT, but no RPE tissue is lost - it is displaced into the excavation.
FCE is typically a benign, stable finding. Several case reports have described a relatively stable course, whether symptomatic or asymptomatic, and after initial evaluation for associated choroidal neovascular changes, it is appropriate to counsel patients on the natural history. Recognised associations include CSCR and, less commonly, choroidal neovascularisation, though these are uncommon and more frequently seen with the non-conforming subtype.
In this asymptomatic young patient with a conforming lesion away from the fovea and normal visual acuity, no hospital review was needed. The diagnosis was communicated to the optometrist by email and the patient was reassured without a hospital visit, returned to routine optometric care with advice to report any new symptoms promptly.
This case is another example of how good quality OCT submitted with a referral can facilitate confident remote diagnosis, meaningful co-management, and an unnecessary hospital visit avoided.